
Dr. Ch. Venkat Kumar Raju, Dr. Sajitha Nair, Dr.C. Jayakumar Amrita Institute of medical sciences Kochi
1 ½ year old child was brought to the ER with complaints of acute onset of swelling involving the face and lips(fig1) which was asymmetric and non-pruritic, there was no edema elsewhere or hematuria. At the time of presentation there is no respiratory distress or stridor, Spo2 was maintained in room air. Chest was clear, general examination was within normal limits. No history of new food or medicine intake.
fig1


fig2
Child was shifted to PICU for observation fearing respiratory distress. Initial routine investigations were within normal limits. At this point we considered the possibility of angioedema ?cause . As there is significant family history of similar complaints(fig3).
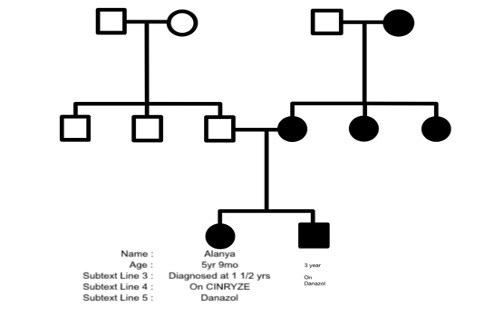
Fig3
a possibility of Hereditary angioedema was also considered. Child was evaluated further. C1 esterase inhibitor levels were low 0.07mg/dl (19-37mg/dl). Whole exome sequencing conformed Heterozygous C.683 deletion in Exon 4 of SERPING 1. Same mutation was confirmed in mother and mother’s siblings also.
Childs acute phase was treated with FFP, and she improved within 24hrs(fig2). Child was discharged and was kept under follow up of pediatrics and genetics department. As child had a Severe angioedema over face and neck with respiratory distress at 2 years of age, she was started on Danazol after explaining the side effects and the need of regular follow up. She was under regular follow up of pediatrics and endocrinology departments. She improved symptomatically with danazol. At 5 years on routine evaluation, she was noticed to have increase in height centiles and advancement in bone age which was considered due to danazol.
. As IV C1 esterase inhibitor was the only one recommended for this child’s age. The process of procuring the drug through the government rare disease policy was initiated .2 vials of the drug was procured, and the parents were counselled to use the drug in case of emergency. The need for prophylaxis therapy with C1 esterase inhibitor was discussed with parents. Supportive care and efforts to protect airways were the main options for managing angioedema until 2009(FFP was exception). Intravenous plasma derived C1 inhibitor was the first new targeted prophylactic therapy approved FDA, later there was Subcutaneous plasma derived C1 esterase inhibitor and human monoclonal inhibitor of plasma kallikrein (lanadelumab). HAE prognosis varies, but with proper management individuals can lead a normal life. Modern therapies improve outcomes, reducing attack severity. Early diagnosis and personalised treatment plans are crucial for favorable prognosis, enabling effective management of HAE impact on daily life. Carry home message- When faced with a child with angioedema having resistance to drugs like adrenaline, antihistamines, and steroids, and with recurrent pattern of attacks with or without family history, consider hereditary angioedema. Routine drugs are ineffective and of no use in a case of hereditary angioedema.