
Dr.Akshay Kishore , Dr.Vaisakh Anand , Dr Sajith Kesavan ,DrC Jayakumar
AIMS KOCHI ,Kerala ,India
One year and 3month old child 1st child of non consanguineous parentage with B.W of 2.6kg with no perinatal problems presented with multiple episodes of non projectile non bilious vomiting of 2 days duration after feeds
There was one episode of generalised jerks lasting for 2 minutes. There is history of two hospital admissions of this one in neonatal period and both episodes had significant metabolic acidosis. Differential diagnosis considered at this point was
1.Mal rotation
2Inborn errors of metabolism
3.Urinary tract infection
4.Faulty feeding
5.GER
6.Meningitis
At admission , child was in shock with cold peripheries and CRT >3.
Blood gas showing pH-7.1 , HCO3 – 11 with significant metabolic acidosis with high anion gap.
Ba was shifted to PICU.
Labs showed significant hypocalcemia also. Ammonia was 78.9 umol/L.
LP study showed high CSF lactate.
USG abdomen was done which was normal.
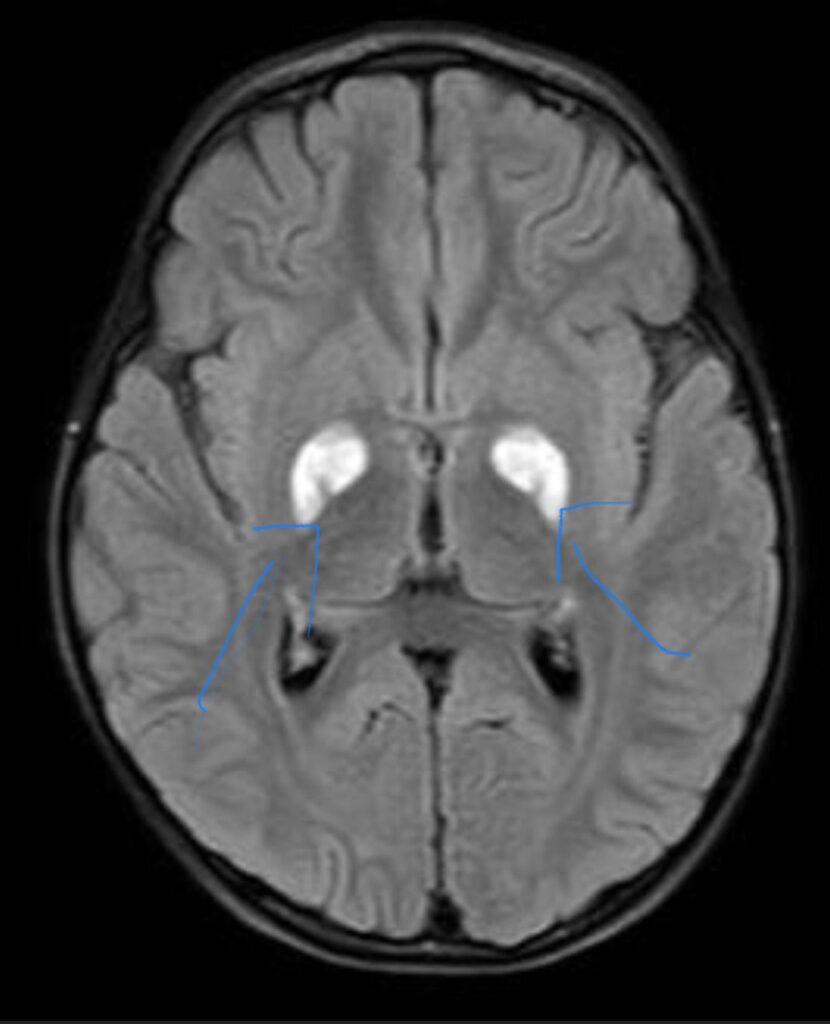
In view of recurrent episodes of vomiting , MRI brain was done.
T2/FLAIR showed bright signals with diffuse restriction in bilateral globus pallidum consistent with organic acidemia.
TMS /GCMS revealed methylmalonic acidemia as the cause of recurrent vomiting leading to significant metabolic acidosis and PICU stay.
Methylmalonic acid levels were sent and it was significantly elevated.
Child was started was started on low protein diet known as the MMA diet after which there was significant improvement.
Discussion : Methylmalonic acidemia (MMA), also known as methylmalonic aciduria is an autosomal recessive metabolic disorder in which the body is unable to process certain proteins and fats properly. This condition was first characterised Oberholzer et al and occurs in one in 48,000 live births. It is caused complete or partial deficiency of the enzyme methylmalonyl-CoA mutase. Diagnosis is based on the high concentration of methylmalonic acid in urine and blood and can also be indicated through the use of CT and MR imaging of the brain.
The most common findings of MMA on imaging is ventricular dilation, cortical atrophy, subcortical white matter abnormality, delay in myelination and abnormalities (T2 high intensity and diffusion restriction) in the basal ganglia, especially in the globi pallidi.
Treatment is low protein diet and to restrict methylmalonic acid.
Prognosis:
Patients with MMA experience significant mortality, and the prognosis for long term survival is poor.
Take home message : Recurrent vomiting in a small ba should be evaluated in a tertiary care centre especially if there is metabolic acidosis and high lactate value to find out the cause and to initiate the treatment as early as possible.