
Dr.Ch.Venkat Kumar Raju, Dr.Suma Balan, (Paed Rheumato)Dr.CJayakumar
Amrita Institute of Medical sciences
Kochi
Kerala
An 8-year-old male child presented with complaints of abnormal gait for the past 1 year. With this complaint child was initially evaluated in a local hospital where a USG hip was done which was normal. MRI Brain showed corpus callosal agenesis and ectopic post pituitary with hypoplastic anterior pituitary- Pituitary stalk interruption syndrome (PSIS)and was found to have central hypothyroidism
(TSH 2.5 /T4 0.7 -3 3)
With the diagnosis of PSIS, he was started on a maintenance dose of steroids
As he has short stature, he was planning on starting GH therapy
In the last few months, the mother noticed persistent gait abnormality and was brought here for further evaluation
On examination- he had a circumduction gait and not bearing weight on his right hip
At this point our Differentials were
1) Avascular necrosis of Hip
2) Osteochondritis
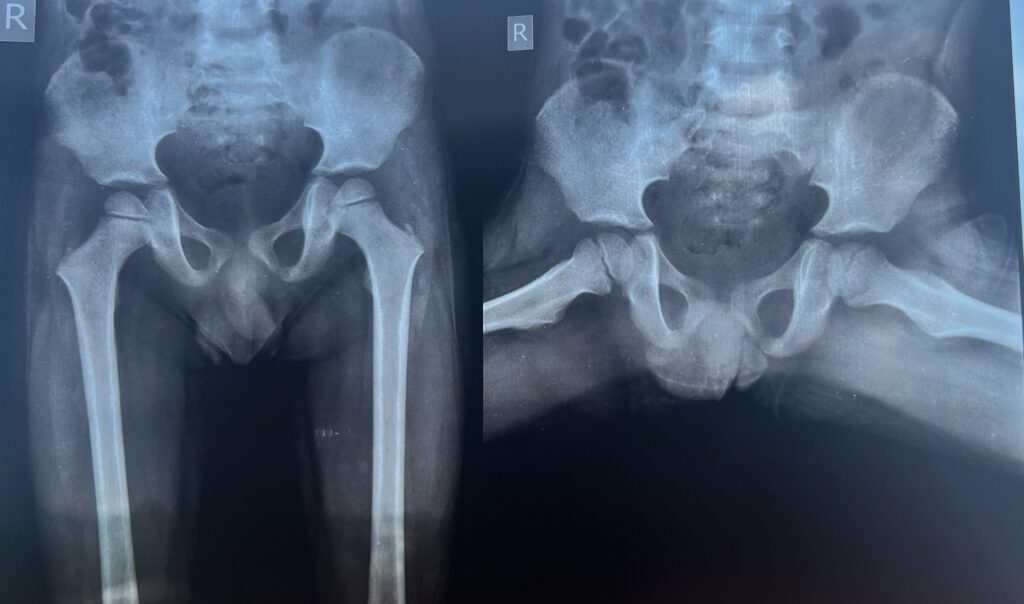
Xray Hip was done
A small sclerotic shadow was observed on the right side on Ishio pubic part of pelvis
Ischiopubic synchondrosis (IPS) is a temporary joint that exists only in childhood, during bone maturation. On occasion it produces pain, whereas on others, it is an incidental finding revealed plain radiography. Given its tumor-like aspect, it is necessary to perform magnetic resonance imaging (MRI) to differentiate it from pathological conditions.
Van Neck-Odelberg disease is a benign process that develops in children between the ages of 4 and 16 years. It is characterized pain in the lower limb due to osteochondritis of the ischiopubic ramus.
There is swelling of the IPS with no clinical manifestations, but it can be associated with pain in the thigh, groin region or buttock, with limitation of the mobility of the extremity and limping. Plain radiography usually shows an enlargement of the synchondrosis with radiolucent and osteolytic areas. The typical MRI findings include changes in bone marrow and perilesional soft-tissue edema.
The tumor-like appearance in radiographs may lead to a diagnosis of stress fracture, an infectious process or tumor.1–5 The absence of fever and normal results on laboratory tests facilitates the differential diagnosis.1
This condition usually has a favorable outcome after 2 or 3 weeks of anti-inflammatory therapy and rest
PSIS is a congenital abnormality characterised a triad of thin or interrupted pituitary stalk, small or absent pituitary gland, and an absent or ectopic pituitary gland. It was first described in 1987 Fujisawa et al and had a reported incidence of 0.5/100 000 births.it is believed to be either due to mutations in the genes involved in pituitary embryogenesis (PROP1, LHX3, HEXSX1, PROKR2 and GPR161) or perinatal asphyxia. PSIS can present with anterior pituitary hormone deficiencies (growth hormone, 100%; gonadotropin, 97.2%; corticotropin, 88.2%; and thyrotropin, 70.3%); however, hyperprolactinaemia (6.9%) due to lack of dopaminergic inhibition can be seen. Posterior pituitary function is intact. These anterior pituitary hormonal deficiencies can present as hypoglycaemia, neonatal jaundice, short stature, cryptorchidism, delayed puberty and micropenis. PSIS is also associated with other midline defects, such as broad nose, cleft lip and palate, single incisor, and nasal aperture stenosis.MRI shows the characteristic triad of absent pituitary stalk, anterior pituitary hypoplasia (98.3%) and ectopic posterior pituitary (91.2%). The ectopic neurohypophysis is most commonly seen in the infundibular recess (60.4%) or the hypothalamus (18.9%).PSIS is a rare condition and international databases need to be established to further study the molecular aetiology.
Take Home message- Van Neck Odleberg disease is rare cause of pediatric pelvic pain. Identifying this disease would let the child undergo less investigations