
Dr Adeena D S , Dr Vinayan KP , Dr Suhas Udayakumar , Dr C Jayakumar Amrita Institute of medical sciences Kochi
6 year old male child with Double outlet ventricle and Ventricular septal defect presented with fever of 10 days ,lethargy of 2 days and 1 episode of generalised seizure. Child was on oral iron & Propranolol, but after 3 yrs only iron was continued as he lost follow-up.
At admission, child was conscious but irritable and saturating his baseline value of Spo2 78%. Neurologically ,he had minimal spasticity in all four limbs and brisk reflexes. He had polymorphous nuclear leukocytosis and CRP of 184 ,Hb of 18.4/ Hct -56%.
ECHO-DORV,large conoventricular VSD, severe valvular and infundibular stenosis. In view of the irritability, MRI brain with contrast was done , that showed multiple well defined round hypo-densities with subdural connection in cerebral convexity.
He was started on IV Ceftriaxone, metronidazole, vancomycin and supportives including anti-epileptics and steroids. In view of persistent fever spikes and recurrence of seizure, CT brain was done(not MRI due to affordability issue), that showed multiple cerebral and right cerebellar abscesses with left subdural empyema.
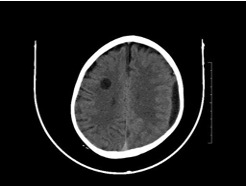

Surgical management of right parietal Burr hole and evacuation done which drained frank pus. Antibiotic was upgraded to Meropenem,but Vancomycin continued. Pus culture was sterile.Child improved following the surgery. Antibiotics was given for a total of 6 weeks as IV 4 weeks followed oral Clindamycin x for 2 weeks. After completion of antibiotic therapy, child is planned for RVOT stenting procedure for the pulmonary stenosis.
Discussion- Intracardiac right to left shunt pass the pulmonary circulation , thus the filtration of lung macrophage is not done effectively and the bacteria reaches the cerebral circulation and forms abscesses.
Take home message- Brain abscess and thrombosis are seen as complications in cyanotic congenital heart disease and any kind of lethargy and irritability may be a manifestation of brain abscess or thrombosis and child should be investigated with MRI /CT head and proper management should be given.
Brain Abscess: 80% of cases are associated with risk factors such as septic contiguous focus, penetrating injuries ,post surgery, right to left shunt lesions. They are most common in frontal lobe ,in TOF-parietal lobe. One third of cases are polymicrobial . Most common organism is streptococcus species. Clinical features include fever headache, irritability, seizures, features of raised ICT, hemiparesis and personality changes. Investigation of choice is MRI brain with contrast. Management is empirical IV antibiotics for 6 weeks-Vancomycin +Metronidazole +/- Ceftriaxone. When suspecting polymicrobial or Gram negative organisms-IV Vancomycin + Meropenem are the antibiotic of choice. It is associated with 5- 10 % mortality and one third cases have sequalae.