
Dr. Venumadhav, Dr.Bhanu Vikraman Pillai (Paed Gatsro) Dr. C. Jayakumar, Dr.Sajitha Nair
Department of Pediatrics, Amrita Institute of Medical Sciences
Introduction
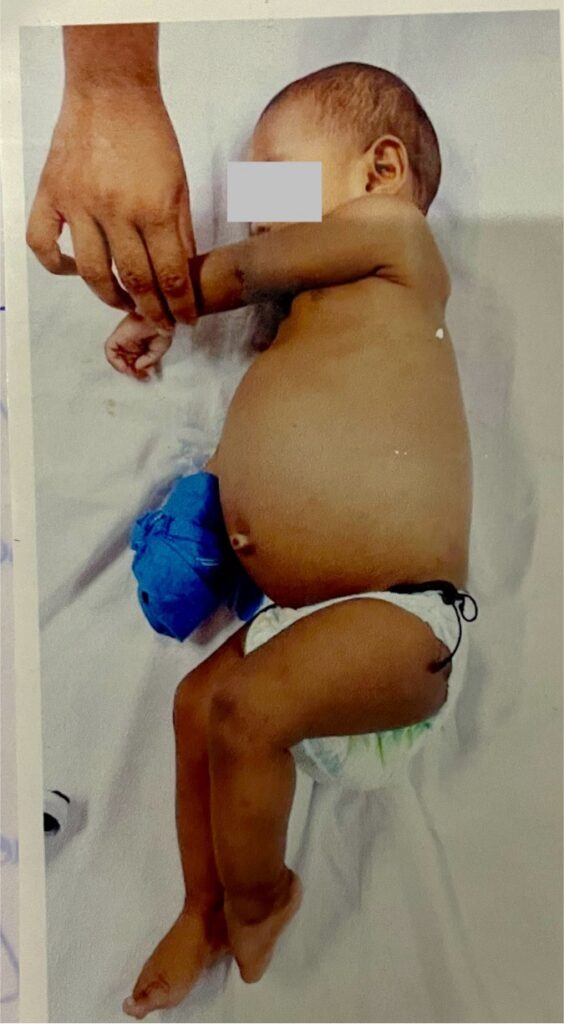
A six month old male child presented to the outpatient department with complaints of progressive abdominal distension over the past 3 weeks,and poor feeding for the past 2 days. There was no history of fever, fast breathing, jaundice, mucocutaneous bleeds, periorbital puffiness, pale coloured stools, intake of indigenous medicines or toxins, irritability, altered sensorium or seizures.
He is born term,AGA, developmentally normal and immunized according to the NIS schedule. He had weight of 6.8Kgs( Between 0 and -2SD), length of 67cms(Between 0 and -2SD) and HC of 41cms(-1 and -2 SD). He has been exclusively breastfed and given complementary feeds of banana and ragi. No family history of liver/ renal diseases/malignancies/ bleeding disorders.
Examination and Investigations:
Child was afebrile with stable vitals. The abdomen was grossly distended with no pallor, icterus, cyanosis, clubbing, lymphadenopathy, or generalized edema. Notable findings included a distended abdomen, everted umbilicus, and distended veins. There was no organomegaly, and the abdominal girth was 52 cm.
Differential Diagnosis:
Chronic Liver disease with portal Hypertension
Right Heart Failure
Thrombophilia Disorders
Budd chiari syndrome
Kwashiorker-Leading to edema
Hepatoblastoma
Chronic hepatitis
Schistosomiasis
Counts were normal (TC-14680, N/L-22/65%, Plt-4.65lakhs) with negative CRP(1.16).URE was normal. There was no proteinuria. LFT showed normal bilirubin,enzymes, ALP and GGT. There was no coagulopathy. However, serum albumin was low (3.2), and D Dimer was normal. Preopserology was negative.
Imaging studies include USG abdomen with doppler done which showed marked ascites and hepatomegaly with altered echotexture. There was inadequate visualization of right hepatic vein, hepatic ostia and IVC with dilated intrahepatic venous collaterals.
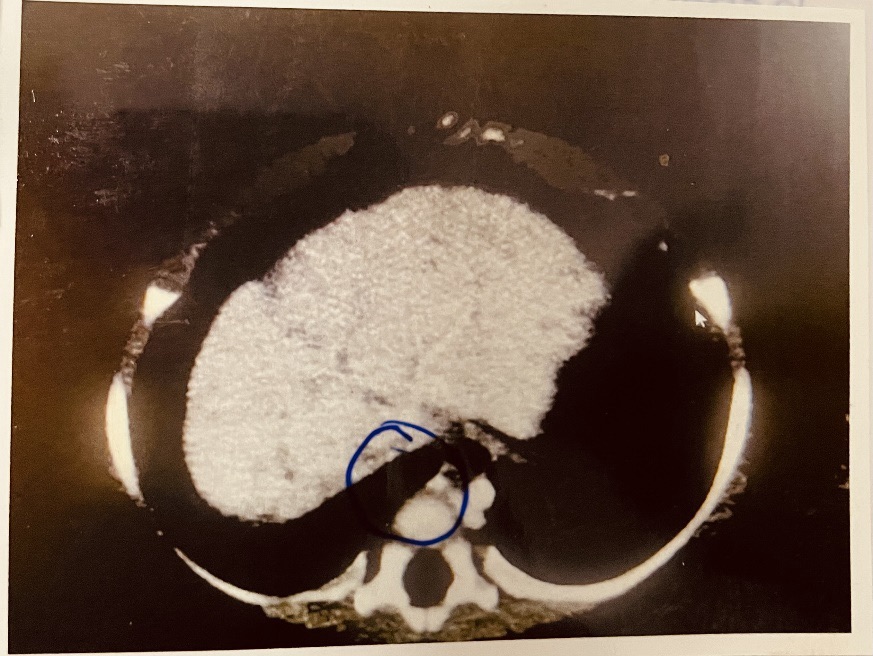
PROMINENT AZYGOUS AND HEMIAZYGOUS SYSTEM
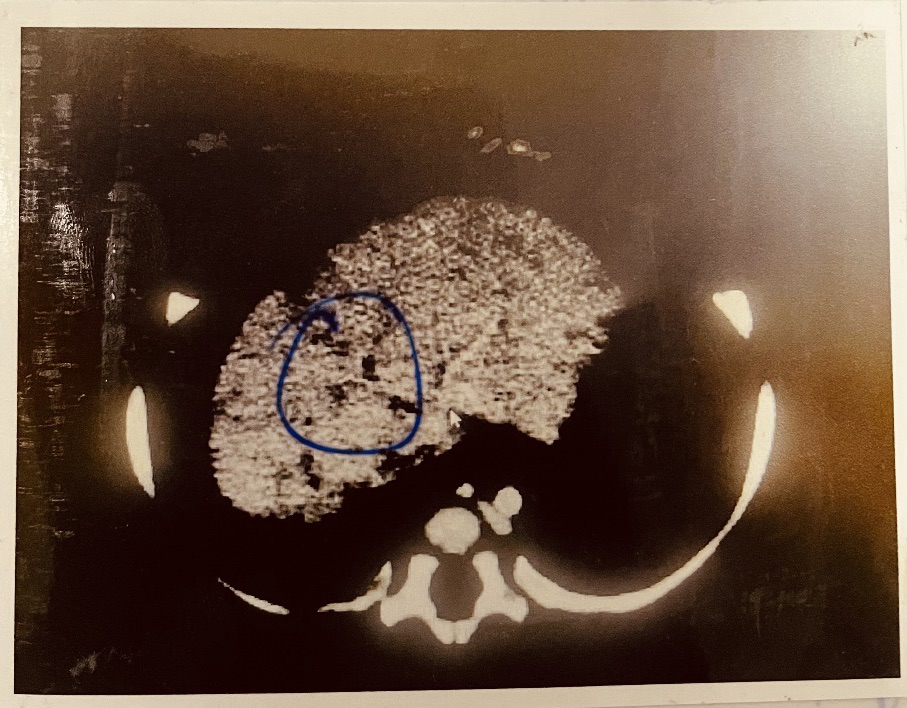
MOTTLED APPEARANCE OF LIVER SURFACE AND NODULARITY

INTRAHEPATIC IVC OSTIUM LIKELY THROMBOSED
Multiphase CT abdomen with contrast showed poorly visualized hepatic veins with thin calibre left hepatic vein,non visualized hepatic vein ostium and intrahepatic IVC-ostium(likely thrombosed) and small calibre short segment of suprarenal IVC.?Budd chiari syndrome of uncertain etiology. Prominent azygous-hemiazygous system were seen decompressing IVC obstruction. Liver showed mottled appearance of with surface nodularity and caudate hypertrophy.
Investigations for prothrombotic states were sent (Proten S-57%,C-59%,Anti thrombin-3 101%and factor 5 leiden-Negative). Tumor markers (CA-19-9, CEA) were negative, with mild elevation of AFP.ECHO ruled out constrictive pericarditis. Primary Immunodeficiency was ruled out relevant investigations. Ascitic fluid was drained after giving 20% albumin. Ascitic fluid analysis was s/o transudate. There were no malignant cells.Blood, urine and ascitic fluid c/s were sterile. Child was started on diuretics (Furoped-10mg/1ml- 0.7ml BD, Tab Aldactone-25mg- mix in 4 ml give 2ml-1ml-0 and LMW heparin(Clexane-0.1ml Subcutaneous, OD).
The dose of diuretics were titrated after monitoring abdominal girth. USG abdomen repeated showed mild to moderate ascites. As there was clinical improvement with stabilisation of abdominal girth, further tapping/pigtail insertion was not done. Parents were taught to administer LMWH. There were also advised to continue medications and review after 2 weeks to plan further management. Child is afebrile and is hemodynamically stable at discharge. Abdominal girth at discharge was 48cms.
DISCUSSION:
Budd-Chiari Syndrome (BCS) is a rare disorder characterized the obstruction of hepatic venous outflow, typically caused thrombosis. This blockage prevents blood from flowing out of the liver, leading to liver congestion and damage. Risk factors include conditions that promote blood clotting, such as polycythemia vera, antiphospholipid syndrome, and other myeloproliferative disorders, as well as oral contraceptive use and pregnancy. Symptoms commonly include hepatomegaly, ascites, abdominal pain, and jaundice, with chronic cases potentially progressing to liver cirrhosis and portal hypertension. Diagnosis involves imaging studies like Doppler ultrasound, CT scans, and MRI to visualize the hepatic veins and identify blockages, alongside blood tests for liver function and clotting disorders. BCS is classified into primary and secondary forms, depending on whether the cause is intrinsic vein problems or external compression tumors or other structures. Untreated BCS can lead to severe complications such as liver failure, esophageal varices, and kidney dysfunction. Treatment options include anticoagulant therapy, thrombolysis, angioplasty with stenting, and liver transplantation in severe cases, often following a step-wise approach starting with less invasive treatments. Early detection and appropriate treatment are crucial for better outcomes. Management should be tailored to each patient and involve a multidisciplinary team, with guidelines suggesting a combination of medical, interventional, and surgical therapies based on individual patient needs and response to treatment.