
Dr.Sruthi, Dr.Sajitha Nair, Dr.C.Jayakumar
Amrita Institute of Medical Sciences, Kochi
Four-year-old presented with high grade intermittent fever (T max- 102`F) and left lower limb pain of two weeks duration. She was initially managed at a local hospital symptomatically and then later with antibiotics (Inj. Ceftriaxone for four days). Persistence of fever and inability to bear weight led referral to AIMS
No history of cough/skin rashes/ pustules were noted. Her perinatal natal developmental and immunisation history were normal
On examination, she was febrile and sick looking with other stable vitals. Auxology revealed weight of 10.4kg (<3rd centile), height of 87cm (<-3SD), MUAC of 13cm, HC- 47.5cm.
Mild pallor was noted. She was not weight bearing on the left leg. Left lower limb was abducted and externally rotated at hip with painful limping. Local rise of temperature was noted with no skin changes. Right lower limb appeared normal. No knee/ankle arthritis noted. Other System examination was normal
Labs CBC normal. CRP of 31.66mg/L and ESR-82mm/hr. Ultrasound scan of the hip
Joint e_usion with echogenic content with maximum thickness of 5mm. Possibility of septic arthritis of the left hip.
She was started on ceftriaxone and Clindamycin.
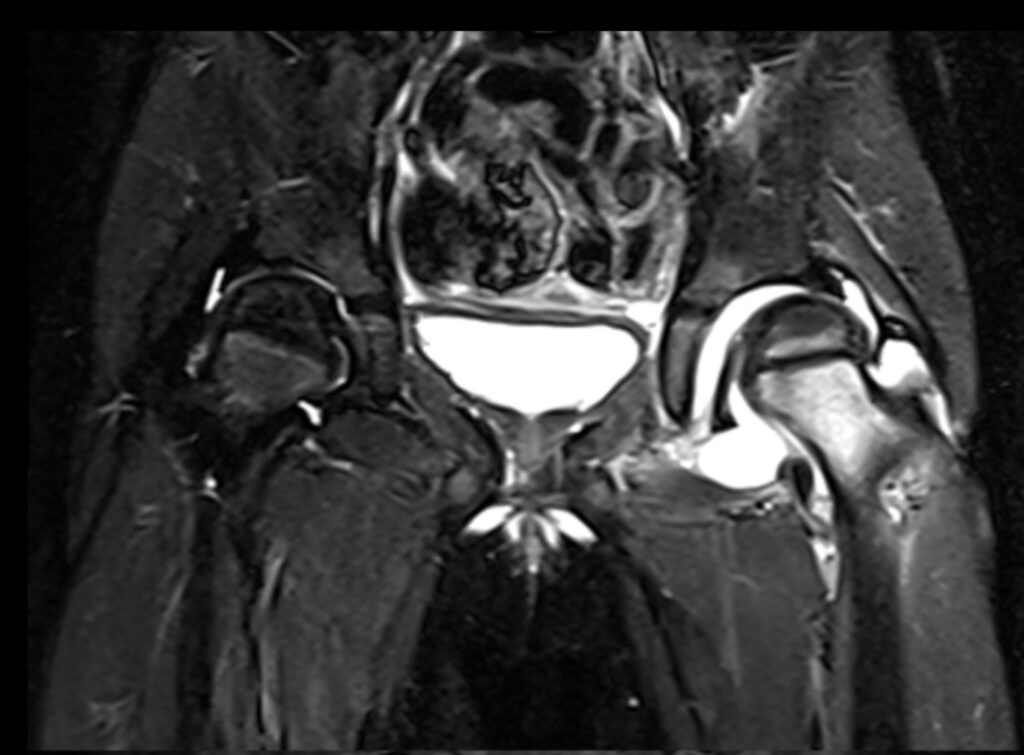
MRI hip with contrast was consistent with septic arthritis. Emergency arthrotomy and debridement of left hip joint was done. The pus from the joint green staphylococcus aureus sensitive to oxacillin, gentamicin, levofloxacin and clindamycin.
As the growth was MSSA, antibiotics were changed to Inj Cefazolin which was given for a total of 14 days. A skin traction was applied, and weight bearing was avoided. In view of short stature she was evaluated and noted to have subclinical hypovitaminosis D for which supplements were started. X-ray wrist showed two carpal bones.
Over the course of hospital stay she remained afebrile and with improving blood parameters she was discharged on oral cephalexin of 4 weeks duration.
Septic arthritis
Septic arthritis is a critical condition bacterial pathogens such as Staphylococcus aureus. The condition necessitates urgent medical intervention due to the potential for rapid joint destruction and severe sequelae. Clinical manifestations typically include acute onset of joint pain, e_usion, erythema, and systemic signs such as fever. The hip and knee joints are predominantly implicated in pediatric cases.
Diagnosis of septic arthritis is multi-faceted, involving a thorough clinical examination, laboratory investigations including elevated inflammatory markers (e.g., CRP, ESR), blood cultures, and radiological imaging. Definitive diagnosis is achieved through joint aspiration and synovial fluid analysis, which may include Gram stain, culture, and PCR for pathogen identification.
Therapeutic management centers on prompt administration of empiric broad-spectrum intravenous antibiotics, tailored subsequently based on culture sensitivities. Surgical intervention, including arthroscopic or open drainage, is often indicated to evacuate purulent material and reduce intra-articular pressure. Early and aggressive treatment is
imperative to mitigate the risk of permanent joint damage and to optimize functional outcomes for the pediatric patient.
Take home message: Early diagnosis, prompt treatment, and multidisciplinary management are essential in cases of septic arthritis to avoid serious complications and to address associated health issues comprehensively.