
Dr Joepaul Joy, Dr Sajith Kesavan(intensivist and Paed pulmonologist), Dr Greeshma Isaac(Intensivist )Dr C Jayakumar
One month old Term/AGA/Female ba born to G3P3L2 mother was referred to AIMS after work up for Tracheoesophageal fistula due to bluishness with initiation of feeds and choking which was turned negative ,but due to choanal atresia and ear anomaly.
At AIMS Ba was started on intragastric feeds which was tolerated well. Gastrograffin study was done and was normal without signs of fistula. Paladai feed was tried under supervision but was not tolerated.
Ophthalmic evaluation showed presence of retinal coloboma Rt>Lft side.
On examination, cry and activity is good, tone is normal.
Vitals showed increased RR of 60/min and peripheral pulses felt. Head to foot examination showed small AF (1x1cm), Coloboma in the eyes, Bilateral low set ears, dysplastic right ear, Left sided choanal atresia, Retrognathia
External genitalia was normal.
Systemic examination revealed murmur in the upper left sternal border turned out to be PDA , mild suprasternal retractions.
Strong suspicion of CHARGE syndrome was considered.
.Cardiac Multi detector computed Tomograhy (MDCT) showed presence of Large PDA and Aberrant right subclavian artery with retro esophageal course. Initially was on diuretics and digoxin. Following which the cardiac status improved and diuretics and digoxin were stopped.Ba underwent PDA ligation.
Ba underwent bronchoscopy under GA which was normal, no TEF.
Ba was on ventilator post bronchoscopy and gradually weaned to bubble CPAP in NICU. In PICU child was put on HFNC due to persistent tachypnoea and respiratory distress.Ba developed neonatal seizures on PND- 11 and was started on levipil.
EEG done showed multifocal epileptiform discharges . Seizures were well controlled after starting levetiracetam.
MRI Brain showed Bony choanal atresia on left side ,Bilateral vestibular dysplasia with absent semicircular canals. Scattered areas of extraaxial bleed along tentorium, falx and in bilateral frontal region.
NSG done later was normal with no evidence of bleed.
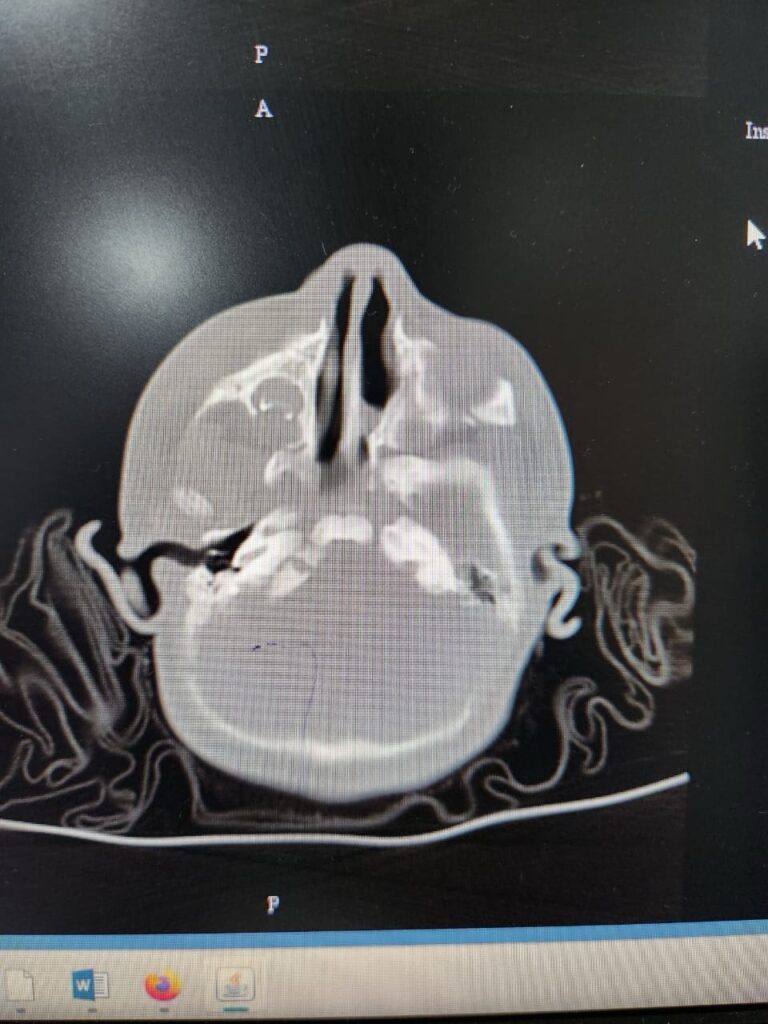
*CT Temporal bone showing left sided choanal atresia
Ba had problems like coagulopathy and jaundice which was managed accordingly .WES could not be done due to financial constraints. Child responded well to the treatment and was discharged with stable vitals.
Discussion- CHARGE syndrome is an inherited disorder caused mutation in the DNA binding protein-7 CHD-7 gene.
CHARGE syndrome is an acronym for Coloboma, Heart disease, Atresia of choanae, Retarded growth and mental development, Genital anomalies, Ear malformations and hearing loss.
It can have high morbidity, but
early diagnosis and treatment life expectancy can be changed . Incidence is in 1/10000 births. Both males and females are equally affected.
Most cases are sporadic and not inherited. Anomalies in neural crest derived tissues can cause CHARGE syndrome.
Diagnosis is initially based on temporal bone imaging and clinical findings. The only gene associated with CHARGE syndrome is CHD7, encrypting the chromodomain helicase DNA binding protein.
Most common neonatal emergencies include cyanosis due to congenital heart defects, or bilateral posterior choanalatresia, less likely due to TEF.
Take home message: Early identification of the syndrome and diagnostic workup to identify individual manifestations will help to prevent the associated complications.