
Dr.Venkatesh Kumar M, Dr.Vinitha Prasad, Dr.Mohan P Abraham (Paed surgeon)Dr.Stefy Sunny , Dr.Shela Sany , Dr.C.Jayakumar
AIMS Kochi
Kerala
India
Eleven year old boy presented with complaints of right sided abdominal pain of one week duration,radiating to thigh and decreased appetite since onset of pain.
He had recurrent right sided abdominal pain and hematuria from 7 –9 years of age which was managed conservatively.
At 7 years of age,USG Abdomen was done which showed Cystitis, Gall bladder sludging, hyperechoic mass extending from dome of UB- likely urachal remnant.
At 9 yrs of age,MCU done showed Grade-3 Vesico ureteral reflux
DMSA showed scarring of Right kidney.
From 9 years of age,he had 6 episodes of Culture positive UTI and was on Cephalexin prophylaxis for 5 months.
General examination was within normal limits.
Auxology revealed normal growth parameters.
Systemic examination revealed tenderness in the right iliac fossa.
Differential diagnosis considered were:
1. Renal calculi
2. Pyelonephritis
3. Chron’s disease
4. Ureteric calculi
5. Malignancies of kidney,ureter and urinary bladder.
INVESTIGATIONS:
CBC: TC-9.72 ku/ml,N-41.3%/L-42.8%, Hb-12.3 g/dl, Plt-527 ku/ml
Urea-17.5 mg/dl,
Creat-0.56 mg/dl
Na+: 132 mEq/L,
K+: 3.5 mEq/L
Pus cells:0-2 /hpf, 5-6 RBC’s/hpf.
Urine culture : Growth positive for E.coli ( More than 100,000cmm )
CECT Abdomen: No significant abnormality.
Cystoscopy done showed multiple purpuric lesions in the bladder and bladder neck and the biopsy was taken .
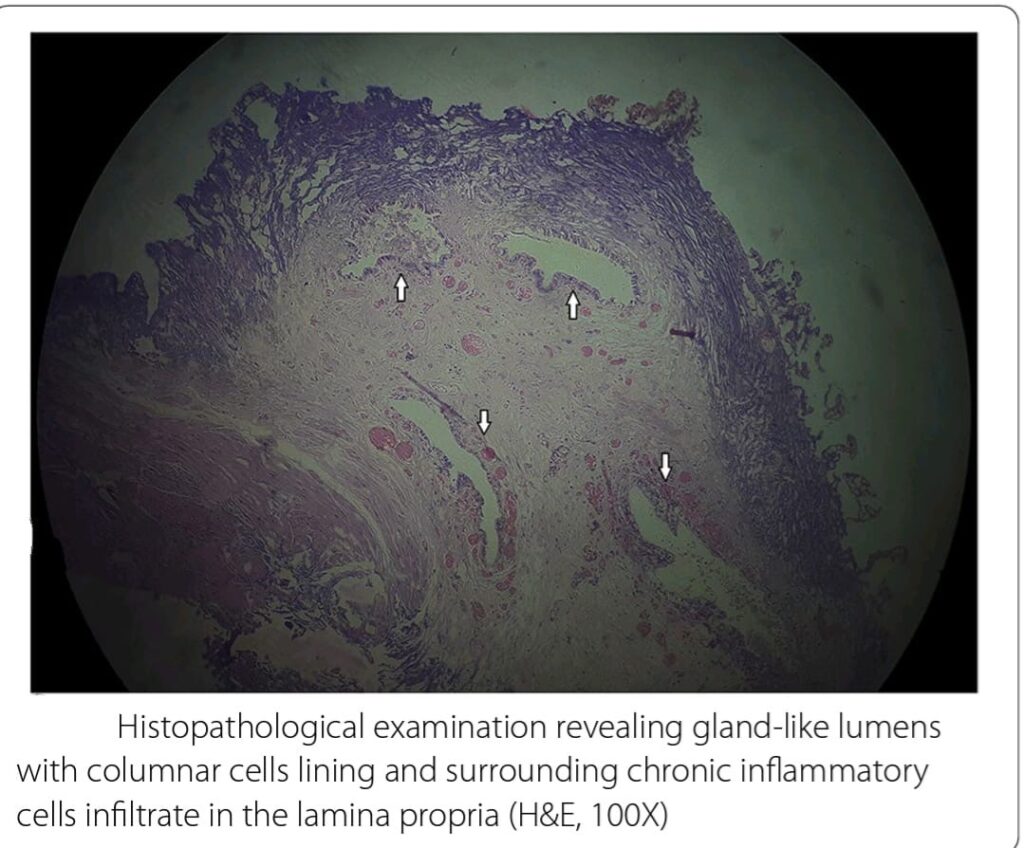
Bladder Biopsy- shows fragments of tissue lined transitional epithelium with lamina propria showing few aggregates of chronic inflammatory cells composed of lymphocytes and occasional histiocytes.
Also noted are few Von Brunn’s nests with some showing secretions within- suggestive of CYSTITIS GLANDULARIS.
No features of dysplasia/Carcinoma in situ /granuloma/parasites noted.
Impression: Cystitis Glandularis
Currently the child is on Syrup Citralka, Tab Acidose (500mg)

Discussion: Cystitis glandularis is a very rare benign proliferative disease of the urinary bladder mucosa. It is usually a microscopic finding and manifests rarely as a large visible macroscopic lesion of UB. Old hypothesis – abnormal embryological development, as per this theory embryonic rests originates from either urachus or intestinal epithelium and get displaced during separation of rectum from urogenital sinus.
Second predominant hypothesis believes it to be a metaplastic change in the vesical mucosa due to inflammation and irritation which leads to formation of Von Brunn’s nest along with degeneration of central cells and metaplasia of surrounding cells to a columnar phenotype which is consistent with cystitis glandularis.
Clinical features: can be asymptomatic, dysuria, increased frequency,urgency, hematuria or mucus in the urine.
Risk factors – bladder exstrophy, pelvic lipohypertrophy, recurrent UTI, inflammation caused urolithiasis, outflow obstruction and indwelling urethral or suprapubic catheter.
Treatment- endoscopic resection of the lesion for symptomatic relief of the patient
For severe and recurrent cases extensive surgical management needed.
Follow up- annual surveillance cystoscopy with bladder biopsy is recommended owing to the transformation to adenocarcinoma.