
Dr.Sruthi, Dr Rema (Paed Haematology), Dr.C.Jayakumar
Dept. Of Pediatrics, AIMS, Kochi
One year old male child of 4th degree consanguineous parentage presented with increasing pallor since 3 months of age.
Born term AGA, uneventful antenatal and post-natal period.
At 3 months of age, during the evaluation of LRTI he was found to have haemoglobin of 1.8gm/dl. He had anaemiainduced cardiac failure and managed with blood transfusion. He had tachycardia at admission and was very pale. He is noted to have hypertelorism, a flat nasal bridge, epicanthal fold and short neck with upturned nose. Auxology revealed wasting and stunting. The head circumference of 45 cm was between 15th-50th centile. He had no organomegaly.

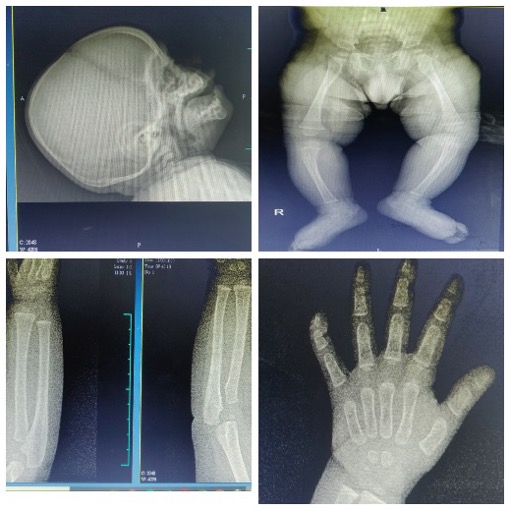
Labs showed normal white cells counts but haemoglobin of 6.7g/dl and platelets of 3,68,000cells/mm3. Peripheral smear showed normocytic normochromic anaemia with thrombocytosis. Ferritin, LDH and coagulation profile were within normal limits. Bone marrow cytology revealed cellular marrow with erythroid preponderance and subtle dyserythropoietic features. Thus, raising a suspicion of congenital dyserythropoietic anaemia. By this time he had 8 blood transfusions in total. Serum folate and vitamin B12 levels were normal. USG abdomen was normal. The skeletal survey showed no evidence of osteoporosis or other abnormalities.
Eye examination revealed no abnormalities. Serum ferritin showed an increasing trend (1288ng/ml), TIBC of 227mcg/dl and serum iron of 225mcg/dl.
Direct Coombs test was negative.
Repeat peripheral smear showed normocytic normochromic anaemia with microcytic hypochromic RBC.
Repeat bone marrow aspiration revealed hypocellular marrow with dyserythropoiesis but the number of binucleated/multinucleated cells were less and inherited bone marrow failure syndromes were thought of.
HPLC could not be done as he had received multiple transfusions.
Fifteen distinct genetic subtypes have been found. All subtypes have an autosomal recessive mode of except FA-B (XR). Nonetheless, a somatic phenotype that is normal or almost normal is present in 25–40% of FA patients. Early Squamous cell carcinoma (SCC) of the head-neck, intestinal or genital tract has an extremely high incidence in FA .FA patients are hypersensitive to DNA cross-linking agents like diepoxybutane, cisplatinum, or mitomycin C. This hypersensitivity manifests itself in the form of excessive growth inhibition, cell cycle arrest, and chromosomal breakage upon exposure to these drugs. Blood transfusions are the best supportive therapy for Fanconi anaemia. Packed RBCs and platelet transfusions have an immediate effect. Cure of aplastic anaemia and prevention of myelodysplastic syndrome can be achieved through bone marrow, peripheral blood cells, and cord blood transplantation. Bone marrow is the preferred method over the others from an HLA-matched sibling. It is essential to do chromosome breakage testing of siblings or other related donors to exclude FA in donors. Gene therapy is a modern developing technique in the management of this disease.
Differentials:
• Dyserythropoetic anaemias
• Congenital aplastic anaemia (Diamond Black fananaemia, Fanconi anaemia, Pearson syndrome),
• Transient erythroblastopenia of childhood
• Orotic aciduria.
Whole exome sequencing was normal. Chromosomal breakage analysis sensitivity to Mitomycin C, hence a diagnosis of Fanconis anaemia was made. They were advised hematopoietic stem cell transplant. However, serial blood transfusions are being given until a suitable donor can be obtained.
Fanconi anaemia (FA):
• Rare inherited syndrome
• Presentations- Short stature, Bone marrow failure, Developmental defects, Gonadal anomalies ,Microcephaly ,Eye anomaly ,Radial and thumb anomaly ,Skin pigmentation, Hearing impairments, Café au lait spots.
An essential message to glean from a case of Fanconi’s anaemia is the imperative for proactive, interdisciplinary care, integrating genetic counselling, vigilant monitoring, and individualized therapies to optimize patient management and enhance long term prognosis