
Dr. Jerin K John, Dr. C Jayakumar
Five month-old first child born on 13 -1-2021 of a non consanguineous parentage, exclusively breastfed,and developmentally normal was referred with generalised lymphadenopathy and massive hepatosplenomegaly (Liver 7cm below the right costal margin and spleen 6cm below the left costal margin respectively )for further evaluation.
Differential diagnosis
1.Thalassemia
Osteoporosis
Neiman pick disease
Gaucher’s disease
Adult type ofCML
Intrauterine infections
At admission, the child was playful and afebrile with other vitals stable. The child was admitted and initial counts (HB6.9gm%Tc- 10 K/ul,N-27%,L-61%,PLT-83 K) showed bi-cytopenia (anaemia and thrombocytopenia). Peripheral smear showed normocytic normochromic anaemia.
RFT was normal.
TB workup was done and was normal.
LDH was mildly elevated.
USG abdomen and CT showed massive hepatosplenomegaly with multiple hypo-dense lesions in the spleen and liver, favouring extramedullary hematopoiesis raising the possibility of leukaemia/lymphoproliferative disorders.
Bone marrow aspiration showed normocellular marrow showing trilineage maturation with 39% mature lymphocytes and prominence of megakaryocytes including hyperlobulated and dyspoeitic forms raising suspicion of myelofibrosis. There were no blast or gaucher cells.
Bone marrow flow cytometry was negative for acute leukaemia.
Lymph node biopsy was suggestive of histocytic sarcoma.
For a second opinion Child was referred to the premier cancer centre in the state and clinical and histopathological diagnosis was agreed up on
But parents opted out for treatment and lost follow up for 2.5 years
They re presented inJannuary 2024
Child was said to have not received any kind of treatment in between
Child was on irregular follow up, latest blood report are normal (Tc-7.97 K/UL,N-32%,L-60%,CRP-0.90 mg/l,PLT-427 K/UL,HB-11.5 g/dl) and peripheral smear showing only thrombocytosis and child is thriving well .GI examination showed spleen of 2cm .Child is asymptomatic and thriving well. The disease has spontaneously resolved without any treatment.
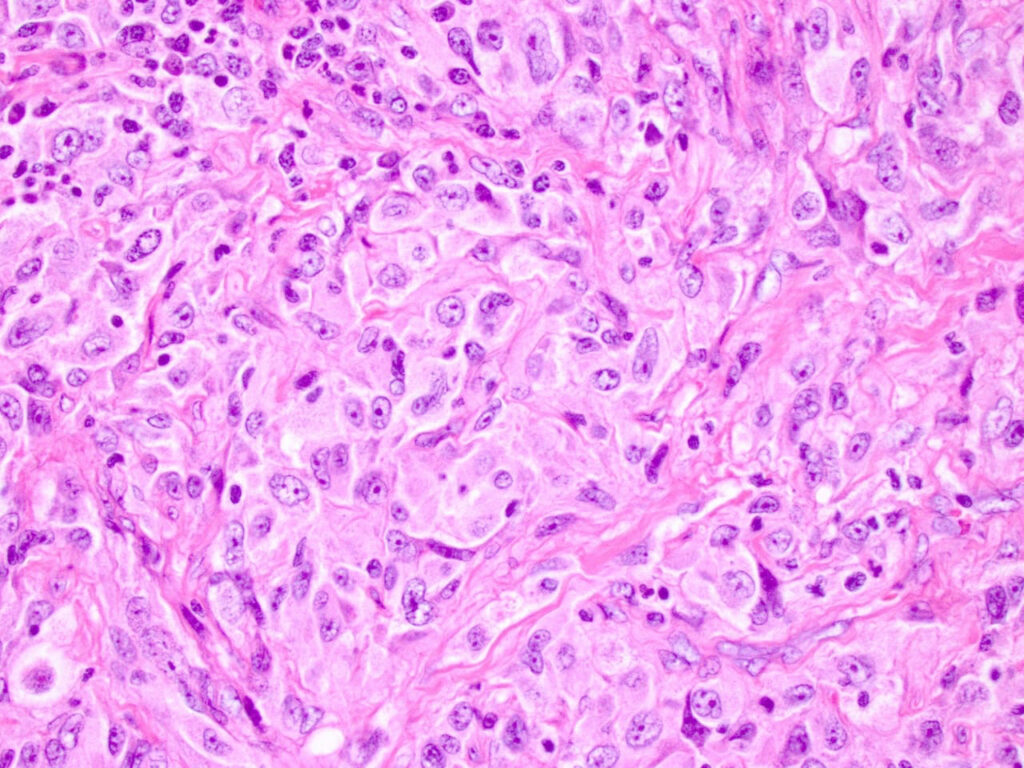
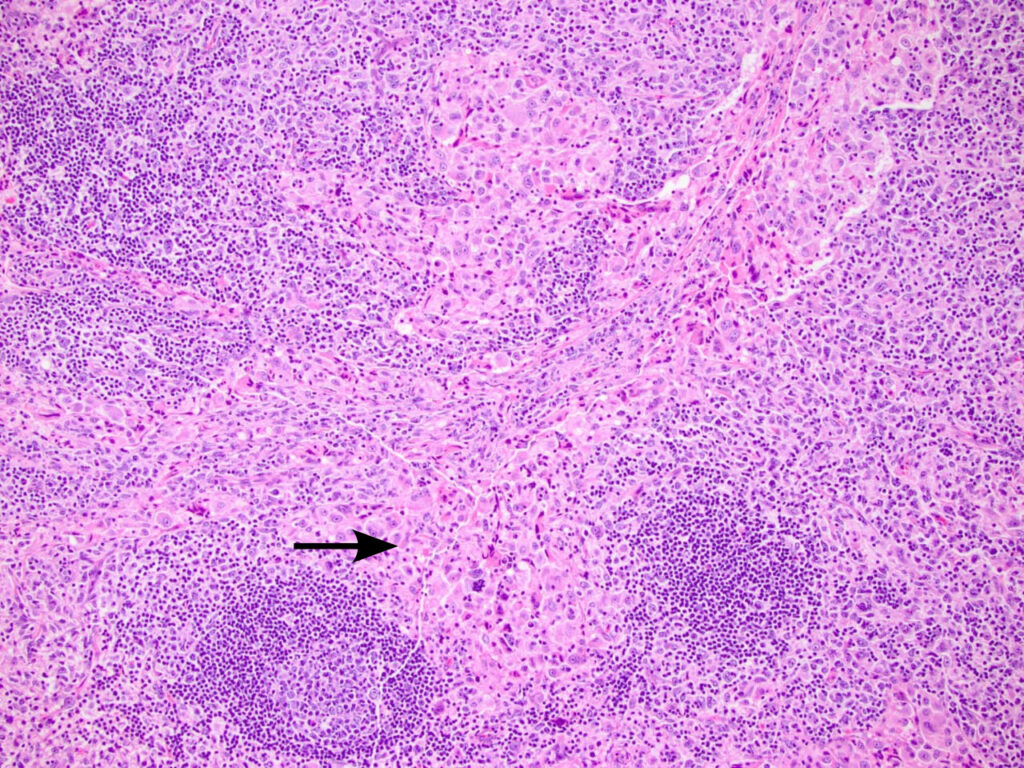
Histocytes
HS is an extremely rare tumour, particularly in children, and accounts for less than 1% of all hematopoietic neoplasms.The pathogenesis of HS arising from other hematopoietic malignancies is attributed to the linear switching of common hematopoietic progenitors due to numerous intrinsic and extrinsic cellular cues that determine their fate. HS most commonly arises in the lymph nodes; however, it may occur anywhere in the body and has been reported in the respiratory tract, gastrointestinal tract, spleen, liver, pancreas, skin, bone and bone marrow, leptomeninges and central nervous system, head and neck, salivary glands, mediastinum, breast, kidney, and uterus. Clinical presentation is usually with advanced disease. Constitutional symptoms are common with fever, sweats, fatigue, weight loss, and weakness. Local symptoms are related to the anatomical area/s affected. Staging requires CT and PET-CT to determine the extent of the disease. Diagnosis is made core, incisional, or excisional biopsy. There is no standardized therapy for HS. Systemic treatments have included regimes for both NHL and Hodgkin lymphoma including cyclophosphamide, doxorubicin, vincristine, and prednisone. Both surgery and radiotherapy have been used successfully as local control measures. Provided the disease is completely resected, outcomes appear to be favourable with recurrence-free survivals of up to 2 years at the time of reporting.
Take home message
This case is a clinical miracle and spontaneous recovery for histiocytic sarcoma has not been reported in the literature.