
Dr Joepaul, Dr Bhanu Vikraman Pillai, Dr Anupa Achamma Thomas, Dr Rekha Hari,
Dr C Jayakumar AIMS Kochi
Three year old male presented with progressive abdominal distension and tiredness for the last one week. He was other wise normal till two years of age.
At that time he had a fall from a bicycle but mother did not consider it as a serious episode. At 2 years and 8 months of age he developed severe abdominal pain and vomiting of 1 day duration.Labs showed neutrophilic leucocytosis with thrombocytosis, elevated lipase and amylase levels. USG Abdomen showed bulky and heterogenous pancreas with mild hypoechoiec peripancreatic collection and mild ascites. CT Abdomen showed Bulky and heterogeneous attenuation of pancreas with peripancreatic inflammation, mild fluid collection in peripancreatic, perisplenic and sub hepatic region and mild ascites- s/o acute moderate severity pancreatitis. He was treated with parenteral Fluids and IV Antibiotics and discharged after 3 days .Thereafter he was doing fine. He had mild abdominal discomfort with fatty meal Two months later he developed progressive abdominal distension and tiredness. Again he had lipase and amylase levels elevation . with sonological evidence of ascites
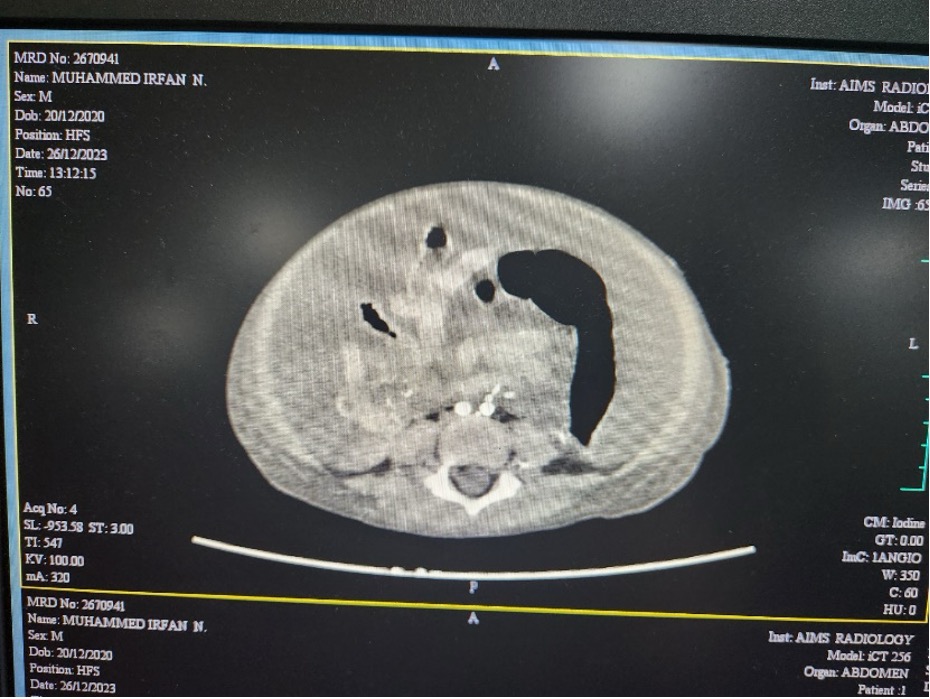
* Abdominal CT showed Mild circumferential thickening with homogenous enhancement of duodenum and short proximal jejunal loop
MRI Abdomen with plain MRCP showed Suspicion of focal discontinuity in pancreatic duct, pancreatic duct obstruction and Significant ascites.
Differentials of Liver cirrhosis, CCF, Nephrotic syndrome, Budd Chiari syndrome were considered. CT Abdomen repeated again showed Mild circumferential thickening with homogenous enhancement of duodenum and proximal jejunum. MRCP showed Suspicion of focal discontinuity in pancreatic duct along anterior aspect of proximal body possibility of pancreatic duct obstruction.
Ascitic fluid analysis amylase value 6000 along with six percentage eosinohils are suggestive of suggestive of pancreatic ascites.He was managed with Cefaperazone Sulbactam ,Inj Octreotide, oral Aldactone and Inj Vitamin K in addition to parental fluids
As Coagulopathy was not corrected with Vitamin K , FFP transfusion was given and taken up for ERCP and Main Pancreatic Duct stenting. He continued to have progressive ascites and hence under aseptic precautions therapeutic ascitic fluid tapping was done 3 times. A CT abdomen was done again following ERCP which showed deficient pancreatic parenchyma in neck region. He was taken up for endoscopy and Naso jejunal tube insertion under anesthesia.Serial monitoring of abdominal girth showed a slow decrease in ascites. Serial monitoring of blood tests also showed an improving amylase value . Antibiotic was downgraded to Inj Ofloxacin after 14 days of Cefaperazone Sulbactam. Infusion pump was arranged prior to discharge and parents were taught about NJ feeds prior to discharge.
Take home message: Blunt trauma of the abdomen should not be considered as simple and imaging and specialists opinion may be sought