
Dr.Ghaniya KC, Dr.Vinitha Prasad, Dr.C.Jayakumar
Two months old male child, presented with complaints of fever and rhinitis since one day.No history of cough/breathing difficulty/ poor feeding/irritability.
No significant past medical history.
1st child of NCM born after reuterine insemination conception.
Antenatal , Natal and postnatal were uneventful
Family history- h/o febrile seizure in mother and uncle
Immunisation history – immunized for age according to NIS schedule.
On examination : child is not sick looking
He is febrile , with other vitals stable
No pallor, icterus,cyanosis, clubbing, lymphadenopathy,edema
Head to foot examination- no neurocutaneous markers or rashes
Systemic examination- normal limits
Rapid antigen test viral panel – negative
Labs – normal counts and negative inflammatory markers.
URE – 0-5 pus cells
Child was started on IV ceftriaxine and other supportives
Over the course of the hospital stay child developed seizures lasting for 2-3 minutes and at the height of fever and was loaded with injection leviteracetam . As a per of the seizure work up one hr Video EEG and MRI brain were done and found normal.
Lumbar puncture was also done and was normal.
48 hrs Urine culture report showed significant growth for enterococcus species.
Ultrasound abdomen showed left ectopic kidney.
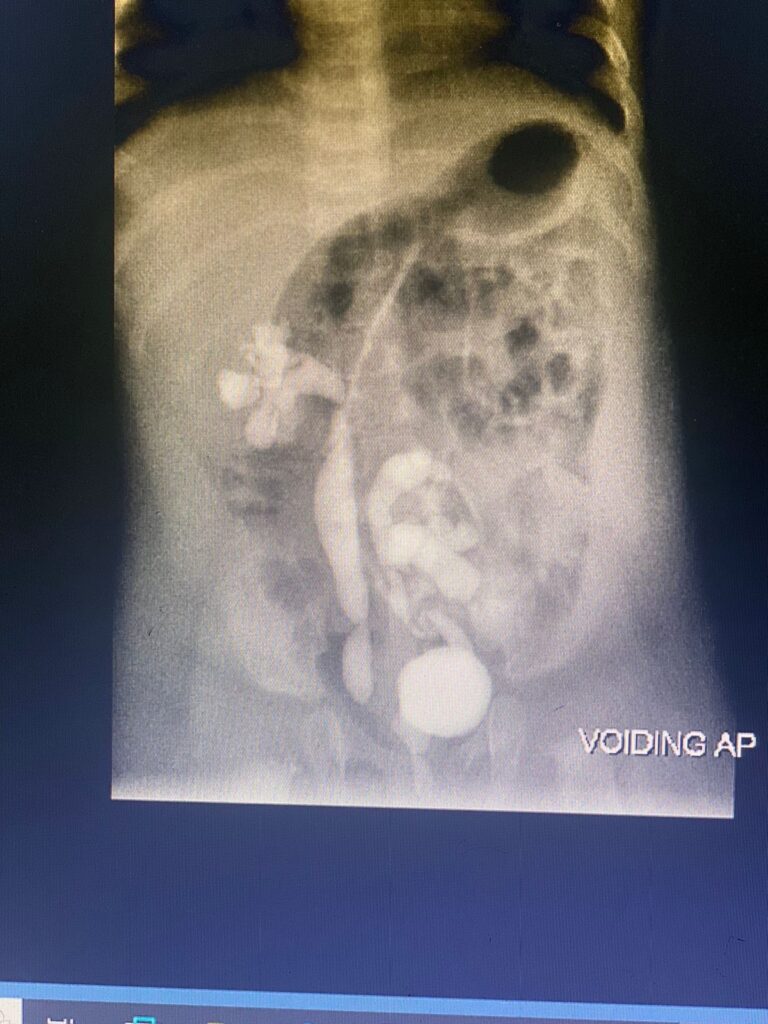
After getting a sterile urine culture , MCU done showed Grade V bilateral VUR , ?PUV.
Cystoscopy + fulguration of the valve circumcision was done after starting cephalexin prophylaxis at 15mg/kg/dose.Cystoscopy confirmed the diagnosis of PUV and left ectopic kidney.

Posterior Urethral Valve (PUV)• Definition: A congenital condition where abnormal leaflets of tissue block or restrict urine flow in the male urethra
Location: The blockage occurs in the posterior urethra, near the bladder neck
Cause: Occurs due to abnormal development of the male urethra during fetal growth.
Gender Affected: Exclusively found in males
Symptoms:• Difficulty urinating or a weak urine stream
• Recurrent urinary tract infections UTIs)
• Enlarged bladder or kidneys (hydronephrosis)
• Abdominal distention.
• Potential kidney damage if untreated.
• Diagnosis:
• Prenatal ultrasound (often shows dilated bladder or hydronephrosis).
• Voiding cystourethrogram (VCUG).
• Cystoscopy.
• Ultrasound postnatally to evaluate the kidneys and bladder.
Treatment:
• Initial Management: Urinary catheterization to relieve obstruction.
• Definitive Treatment: Endoscopic ablation or resection of the valves via cystoscopy.
• Long-Term Management: Monitoring kidney function, possible use of antibiotics to prevent UTIs.
• Complications:
• Chronic kidney disease (CKD) or renal failure.
• Bladder dysfunction or incontinence.
• Urinary reflux (vesicoureteral reflux)
Prognosis: Depends on the severity of the obstruction and the extent of kidney damage; early detection and treatment improve outcomes.