
Dr Varsha V S, Dr C Jayakumar,DrPraveena drNavya George Dept of Pediatrics , Amrita institute of medical sciences.
Four years 5 month old developmentally normal previously asymptomatic female child presented with complaints of on and off high grade fever of 2 weeks duration associated with generalized fatigue and leg pain.History was negative for any other significant symptoms . Child was febrile, sick looking, irritable and pale with stable vitals. Periorbital puffiness was present and Bone tenderness elicited over the supraorbital region . There was no significant lymphadenopathy. Abdominal examination showed splenomegaly of 5cm below the left costal margin .Haemogram showed leucocytopenia (TC: 2.07K/uL) with neutropenia(ANC:124.2), thrombocytopenia (Plt- 7000) and anemia (Hb: 7.7g/dl). Other biochemical parameters done were: LDH(3436U/L)/ S. Ferritin(1575ng/ml) were elevated. LFT/ RFT/ S, Electrolytes/ PT- INR/ APTT/ Lipid profile/uric acid were within normal limits. PS done showed Microcytic hypochromic RBC with elliptocyte, few large lymphoid cells with no blast and thrombocytopenia. USG abdomen done showed mild splenomegaly. Differential considered were Aplastic anemia, Myelodysplastic syndromes, Acute leukemia, Fanconi anemia and Infectoius mononucleosis due to Peri orbital puffiness Child was given 10ml/kg of packed red cells and one unit of platelet transfusion. In view of severe thrombocytopenia ophthalmology consult was sought to rule out fundal hamarrohages .Bone marrow aspiration done revealed 84% blasts hence a diagnosis of acute leukemia was made.
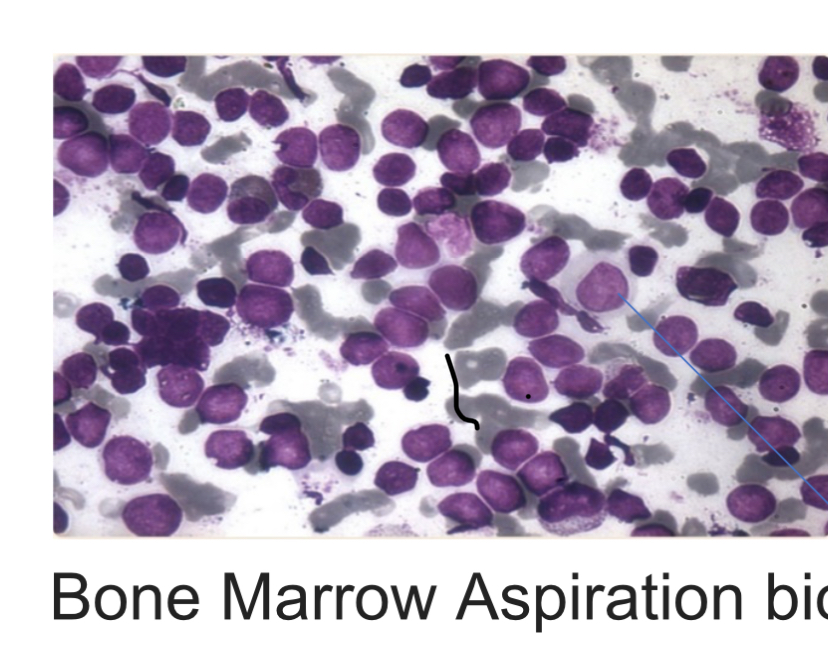
Bone marrow Aspiration showing blast cells.
Flow cytometry showed CD10 Positive B-Cell Acute Lymphoblastic Leukemia. Bone marrow biopsy showed crushing and fragmentation of marrow spaces. Sheets of atypical cells with scant cytoplasm ,monomorphic round nuclei with vesicular chromatin and conspicuous nucleoli. – Other marrow spaces show few hematopoietic elements, consist of erythroids in normoblastic maturation , maturing myeloids with normal morphology and scattered megakaryocytes.Child was managed as per the BFM protocol
Acute lymphocytic leukemia (ALL) is a malignancy of B or T lymphoblasts characterized uncontrolled proliferation of abnormal, immature lymphocytes and their progenitors, which ultimately leads to the replacement of bone marrow elements and other lymphoid organs resulting in a typical disease pattern characteristic of acute lymphocytic leukemia.. Leukaemia children patients typically present with symptoms of night sweats, easy bruising, skin pallor, unexplained lymphadenopathy, weakness, weight loss, hepatosplenomegaly, or difficulty breathing. Bone pain, mental changes, and oliguria may also be present. ALL can also present with testicular enlargement, musculoskeletal pain, mediastinal mass, and incidentally found peripheral blood cell abnormalities. Diagnosis of B cell ALL/LBL requires detection of lymphoblasts with the characteristic immunophenotype in peripheral blood, bone marrow, or other involved tissue. Prognostic, factors for ALL includes age, initial count gender, cytogenetic abnormalities. Management includes combination chemotherapy followed stem cell transplant.
Carry home message
Even if the peripheral smear is not suggestive of ALL , Bone marrow examination is a must in all suspected cases
Never start steroids before one confirm the diaganosis Bone marrow aspiration and Biopsy. Overall survival rates of ALL varies from 45% to 81% (commonly >60%) and event-free survival ranged from 41% to 70% (commonly >50%). Usual follow up of a child with ALL with out relapse include monthly visit for the first 6 to 12 months then every 3 to 6 months for the next 4 yrs and yearly after that.